|
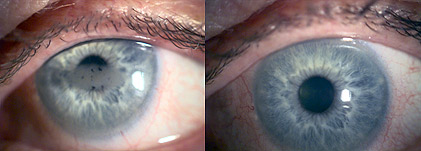
This is a therapeutic application of Excimer laser in the management of
anterior corneal diseases and is a
new technique of Keratectomy for removing the scar tissue from the cornea.
The excimer laser may provide a
novel modality in the treatment of a number of superficial corneal
disorders. This treatment is known
as Phototherapeutic Keratectomy. The indications include a variety of
corneal degenerations and
dystrophies, corneal irregularities, and superficial scars. While some of
these conditions, could be treated
by mechanical superficial Keratectomy techniques, PTK may minimise tissue
removal and surgical trauma. The
smooth stromal surface achieved by the excimer laser procedure may improve
surface quality of the cornea,
improve postoperative corneal clarity and decrease postoperative scarring
and facilitate subsequent epithelial
adhesion. Moreover superficial corneal disorders, which in some cases would
otherwise require corneal
transplant, may be amenable to treatment with the PTK procedure. Thus PTK
has a dual approach in pain
management and improving the visual acuity (removing scars).
Unlike LASEK or LASIK technique for correction of refractive errors, PTK
treatments will vary with different corneal disorders and the clinical goals
of the procedure may likewise vary depending upon the patient's symptoms.
Background of PTK
Historically anterior corneal diseases were managed medically by means of
lubrication, bandage contact lenses or surgically by performing anterior
stromal micropunctures, epithelial debridement or automated
lamellar/penetrating keratoplasty. During the last 10 years the advent of
the excimer laser has become a useful tool for therapeutic reasons, although
is principally focussed on refractive surgery.
PTK Technique
The technique dependes upon the type and distribution of the pathology.
- Large area photoablation
- Focal Ablation
- Smoothening Technique
- Transepithelial
- Basement Membrane Ablation
- Manual Superficial Keratectomy combined with large area PTK
- PTK with masking fluids
- PTK with PRK
Post-PTK management
- Bandage Contact Lens
- Antibiotic eye drops
- Analgesia
- Sedation
- Dark glasses
Complications
Following laser most patients will experience some amount of pain/discomfort
for two to three days. Photophobia (light sensitivity) may continue for a
couple of weeks.
Occasionally there will be a delayed healing up to 7 to 10 days.
There is always very small risk of infection.
In deeper ablations there will be some amount of Corneal haze which may persist for a few months.
There is a tendency for patients to go longsighted/shortsighted after
treatment.
Sometimes dystrophic conditions may recur.
Clinical Outcomes of Phototherapeutic Keratectomy
Bristol Eye Hospital, Bristol, U.K.
Mundasad, M.V., Ross, A.H., Tole, D.M.
Abstract
To evaluate the outcome of Phototherapeutic keratectomy (PTK) in the
management of anterior corneal diseases.
Setting Bristol Eye Hospital, Bristol/Optimax Laser Eye Clinic
Methods
A retrospective review of all patients who underwent PTK between March 2001
until November 2003 for anterior corneal diseases. Patients were assessed as
to whether the indication for PTK was for visual improvement or for ocular
surface improvement, and hence divided into a Visual group and Non-Visual
Group.Further data including pre and postoperative unaided VA, BCVA,
ablation depth, spherical equivalent and complications were collected. In
addition, patients within the Non-Visual Group were contacted recalled to
determine whether they had further symptoms.
Results
A total of 39 eyes of 29 patients underwent PTK for various corneal
disorders. In the visual group, there were 19 eyes of 14 patients and in the
non-visual group 20 eyes of 15 patients.Within the visual group, the BCVA
remained stable or improved in 100% of the group. 10 eyes had stable
post-operative refractions, 6 developed a hyperopic shift and 3 had a myopic
shift. Of the eyes in the non-visual group, 80% had significant improvement
in symptoms.
Conclusions
Phototherapeutic keratectomy is a valuable technique in treating
recalcitrant anterior corneal disease for both visual improvement as well as
symptomatic relief.
Introduction
The advent of the excimer laser has brought about a new method in the
treatment of anterior corneal diseases and smoothing surface irregularities.
Apart from various types of keratoplasty, existing treatment modalities for
anterior corneal diseases include lubricants, bandage contact lenses,
stromal micropuncture as well as epithelial debridement.1
Here, we describe the results of our experience in Phototherapeutic
Keratectomy (PTK) for the treatment of a diverse range of anterior corneal
pathology.
Patients & Methods
Thirty-nine eyes of 29 patients who had Phototherapeutic Keratectomy (PTK)
for various anterior corneal diseases (Table 1) in Bristol between March
2001 and November 2003 were analyzed. The patients had been refractory to
other forms of treatment. All had attempted use of ocular lubricants, 16 had
tried a bandage contact lens, 3 had micropuncture, 3 had epithelial
debridement and 2 had received a corneal graft prior to PTK.
All procedures were performed by a single surgeon (MV Mundasad). Patients
were assessed as to whether the indication for PTK was for visual
rehabilitation (Visual Group) or to alleviate symptoms such as pain and
discomfort (Non-Visual Group).
The preoperative and postoperative examinations included uncorrected and
best corrected visual acuity, spherical equivalent, as well as subjective
symptoms within the Non-Visual Group. Laser ablation depth, complications as
well as number of clinic visits pre- and postoperatively were also noted.
Subjective symptoms were assessed via an initial letter as well as a
follow-up telephone questionnaire.
All treatments were performed with a NIDEC EC5000 laser, using an optical
zone of 6.5mm and a transition zone varying between 7.5 to 9.0mm.
Postoperative management consisted of an eye pad, topical antibiotics,
sedatives and NSAIDs.
Treatment was carried out on an outpatient basis and there was a minimum
clinic follow up of 3 months.
Table 1. Preoperative corneal diseases
| Visual Group |
Number of Eyes |
| Band Keratopathy |
8 |
| Reis Bucklers |
8 |
| Corneal Scar |
2 |
| Lattice Dystrophy |
1 |
| Non-Visual Group |
Number of Eyes |
| Basement Membrane Epithelial Dystrophy |
12 |
| Bullous Keratopathy |
6 |
| Erosions secondary to trauma |
2 |
For 2 eyes, Phototherapeutic Keratectomy was combined with Photorefractive Keratectomy (PRK).
Results
Thirty-nine eyes of 29 patients were treated with PTK for various anterior corneal diseases.
Visual Group
In the visual group, there were 19 eyes of 14 patients. Within the group, age ranged from 13 to 89 years with a mean age of 62 years. BCVA was improved or unchanged in 19 eyes (100%) of the visual group. Figure 1 shows the gain and loss of BCVA within the visual group at follow up.
Visual Group: Gain/Loss Sneilen BCVA
Non Visual Group
In the non-visual group, there were 20 eyes of 15 patients. Age ranged from
27 to 89 years, with a mean age of 55 years. Although, not the primary
indication for PTK treatment within the non-visual group, BCVA was improved
or unchanged in 16 eyes (80%) of the group. Two eyes had a loss of 1 snellen
line and 1 eye lost 4 snellen lines at follow up, secondary to a branch
retinal vein occlusion.
A mean ablation depth of 70 microns was used for eyes with a diagnosis of
bullous keratopathy and a mean ablation depth of 12 microns was used for
eyes with corneal erosion syndrome.
2 eyes with corneal erosion syndrome received photorefractive keratectomy
(PRK) in combination with the PTK resulting in 6/6 snellen vision in both
eyes.
80% of the non-visual group had no further symptoms of pain and discomfort
at a period of 6 months to 3 years following initial treatment. 1 patient
had further symptoms post laser requiring a second PTK treatment.
Out of the 20 eyes, there were 6 cases of haze at follow up, all graded as
0.5 on a haze scale.
Discussion
Within the UK, phototherapeutic keratectomy is in many respects still in
the early stage of development. It is still not widely available for
treatment for anterior corneal diseases in many health authorities.
A good outcome of PTK depends on careful patient selection, detailed
pre-operative evaluation as well as the skills and technique of the PTK
procedure itself.
The success of excimer laser corneal surgery depends on its ability to
remove corneal tissue without resulting in significant collateral damage.
The main adverse effect from PTK is postoperative refractive changes.2
All types of refractive change can occur but the greatest risk is of
hyperopic shift3, due to central flattening of the cornea, which is related
to ablation depth.
In our study, within the visual group, we achieved an overall success
rate of 100% in improving BCVA. With regard to the non-visual group, our
experience suggests that PTK is an effective treatment in alleviating
symptoms of pain and discomfort, with improvement of symptoms in 80% of
cases. Within the latter group, it was noted that many of these patients had
a measurable improvement in Snellen Visual acuity. This most likely
represents a more stable corneal epithelium and decreased photophobia.
It was noted that 3 patients within the visual group had a small myopic
shift. This was thought to be due to uneven laser energy distribution due to
prolate shape of the cornea, effect of plume, as well as possible unreliable
prelaser refraction.
On the basis of our results, we conclude that PTK is an effective
procedure in treating a diverse range of recalcitrant anterior corneal
diseases.4 Not only does it have the ability to improve vision but also to
alleviate symptoms of pain and discomfort.
Excimer laser PTK is a safe and effective modality, providing an
alternative to procedures such as lamellar or penetrating keratoplasty in
certain anterior corneal diseases.
- Hykin PG, Foss AE, Pavesio C, Dart JKG. The natural history and management of recurrent corneal erosion: a prospective randomized trial. Eye 1994; 8:35-40
- Gartry D, Kerr Muir M, Marshall J. Excimer laser treatment of corneal surface pathology: a laboratory and clinical study. Br J Ophthalmology 1991; 75:258-269
- Dogru M, Katakami C, Yamanaka A. Refractive changes after excimer laser phototherapeutic keratectomy. J Cataract Refract Surg 2001; 27:686-692
- Fagerholm P, Fitzsimmons TD, Orndahl M, Ohman L, Tengroth B. Phototherapeutic keratectomy with the excimer laser: long-term follow up results in 166 treated eyes. Refractive and Corneal Surgery 1993; 9:S76-81
|